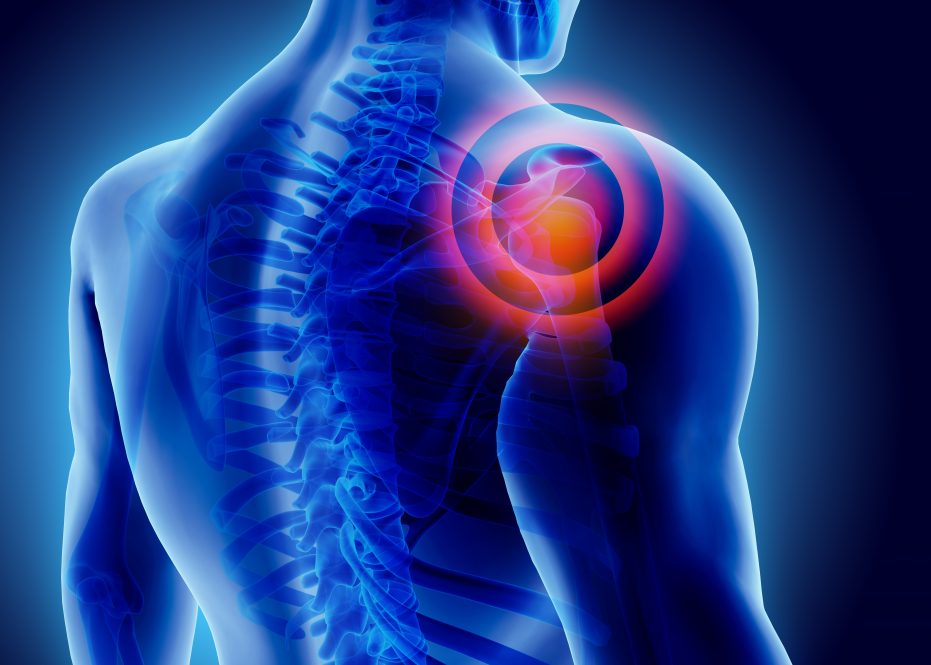
Ever hear of your glenohumeral joint? Probably not.
But it is the critical ball-and-socket joint helping you use your shoulder daily. In fact, the shoulder is most mobile joint in your body. However, the joint’s increased mobility also makes it the most unstable and commonly dislocated.
The shoulder joint is comprised of the socket, which looks like a golf tee, and the upper part of the arm, the humeral head, which looks like a golf ball. Injury to shoulder ligaments and labrum can often render the shoulder joint unstable. Plus, multiple dislocations can wear away the glenoid much like losing the edge of a golf tee. This bone loss makes the shoulder even more unstable.
“Bone loss is a very significant part of the problem,” says UConn School of Medicine’s Chief of the Division of Sports Medicine Dr. Robert Arciero, who was in the military early in his medical career, where he first learned shoulder instability is actually more prevalent than ACL knee injuries.
The amount of bone loss a patient has in their shoulder actually changes the surgery a patient requires. Also, if bone loss in the shoulder joint is not treated it can lead to failure after a less invasive procedure, such as an arthroscopic repair.
Coracoid bone graft transfer has been the gold standard used by orthopaedic surgeons to address bone loss and to stabilize the shoulder joint. The coracoid is a local graft in the shoulder taking a piece of a patient’s own shoulder blade and transferring it to the front of their shoulder socket. This longstanding technique helps hold the ball in the socket of the shoulder joint to stop the joint’s future dislocation.
While other alternative bone transfer techniques using a patient’s own localized bones have been used, Arciero and colleagues concluded in the March issue of the American Journal for Sports Medicine that coracoid transfer remains the most reliable restorative bone graft option for shoulder surgery repair. Also, it is the only technique capable of filling a large glenoid joint defect of up to 40%.In the study, the researchers stratified the percentage of bone loss that can be restored by each of the three localized bone grafts techniques for shoulder surgery repair: coracoid, distal clavicle and scapular spine.
“This is first time in literature that we have compared three local autografts,” says Arciero and co-researchers who report one technique still has the strongest advantage.
Listen to AJSM’s podcast with Dr. Robert Arciero and colleagues discussing their findings.
“The history,” says Arciero, regarding the coracoid bone graft. “This option was invented or described in 1954. That means there is almost 70 years of clinical data on its use. That’s a huge advantage to using the caracoid. It works! But there is a steep learning curve.”
Arciero adds: “As far as coracoid, our study results match previous research work.”
The research team looks forward to more clinical data becoming available overtime for the other alternative bone graft techniques currently leveraged by orthopedic surgeons.
According to Arciero, the new study findings are a true game changer for orthopedic surgeons, and even his own surgical practice.
“The caracoid can be used for larger glenoid bone defects. That’s the take home message that’s changing my practice,” says Arciero. “We found that you can definitely go up to 30 percent [for a glenoid defect repair need] and still achieve sufficient solution to the glenoid bone loss with just the caracoid.”